Infinity Communication Access Lab Recognized With 2012 Product Utilization Support and Help (PUSH) Award

TECHNICAL BRIEF NO. 36 - 2013
A Publication of SEDL's Disability Research to Practice Program
Infinity Communication Access Lab Recognized With 2012 Product Utilization Support and Help (PUSH) Award
James A. Leahy, BS, Center on KT4TT, University at Buffalo (SUNY)
Tom Chau, PhD, PEng, Bloorview Research Institute
This FOCUS Technical Brief describes the exemplary knowledge translation work of the winner of the Center on KT4TT's 2012 PUSH Award. The recipient, Infinity Communication Access Lab, is a partnership between Holland Bloorview Kids Rehabilitation Hospital and the Toronto District School Board in Toronto, Canada. The lab aims to discover person-centered access solutions and to ensure that those solutions are transferred into environments true to where children live and learn. Dr. Tom Chau oversees the lab, which serves 130 public school students with a range of developmental conditions.
2012 Product Utilization Support and Help (PUSH) Award
The Center on Knowledge Translation for Technology Transfer (KT4TT) is pleased to announce that Dr. Tom Chau and the team at the Infinity Communication Access Lab are the recipients of the 2012 PUSH Award. Dr. Chau is vice president of research and director of the Bloorview Research Institute, Holland Bloorview Kids Rehabilitation Hospital, University of Toronto. He is also the Canada Research Chair in Pediatric Rehabilitation Engineering as well as a professor at the Institute of Biomaterials and Biomedical Engineering, University of Toronto.
Dr. Chau and his team exemplify knowledge translation for technology transfer by implementing a need-driven approach to each new clinical intervention, while keeping in mind the broader linkages among scientific research generating conceptual discoveries, engineering development generating prototype inventions, and industrial design and production generating product/service innovations.
The Holland Bloorview-Toronto District School Board Infinity Communication Access Lab (Infinity Lab) has conducted exemplary work in three areas related to knowledge translation for technology transfer, each of which is referenced in the following project summary.
- Establishment of a multi-institutional community of practice to address communication needs of children with developmental disabilities such that knowledge about the child, the prescribed technology, and the individualized communication strategies flow naturally and continuously among members of the community, facilitating need identification, technology prescription, technology adoption, and consistent implementation across settings.
- Development of a comprehensive training and measurement regime that translates new knowledge from research to parents, teachers, therapists, and clients throughout the access journey from need to product.
- Building of an evidence base for client- and family-centered access innovations that harness the unique personal abilities of each individual client, ensuring that practice wisdom is codified alongside rigorous and empirically generated knowledge.
Background
The Infinity Communication Access Lab arose as a partnership between the Holland Bloorview Kids Rehabilitation Hospital and the Toronto District School Board. These partners are, respectively, the largest pediatric rehab hospital and the largest school board in Canada in terms of the number of clients and students served in a single year. Holland Bloorview is also a fully affiliated teaching hospital of the University of Toronto, serving 7,000 children with disabilities each year, with about 600 inpatient admissions and 58,000 outpatient visits.
This "living" lab is situated inside Sunny View Public School, a junior school (grades 1–8) within the Toronto District School Board. Sunny View has 130 students with a range of developmental conditions (e.g., spastic quadriplegic cerebral palsy, autism, various encephalopathies, genetic disorders, muscular dystrophy). Many of the students have a limited communication function, which in turn restricts their participation in the school curriculum and their development of social skills and language.
The Infinity Lab was created as a multi-institutional partnership to address this communication challenge. Specifically, the lab aims to discover person-centered access solutions and to ensure that those solutions are transferred into the actual environments where the child lives and learns.
Need-Driven Knowledge Ecosystem
Knowledge translation activities of the lab are rooted in the framework of a need-driven knowledge ecosystem (Chau, Moghimi, & Popovic, in press). In this ecosystem, the key process is the flow of knowledge among three related states: conceptual discovery, prototype invention, and product/service innovation (Lane & Flagg, 2010).
For the Infinity Lab, the initial inputs to the ecosystem are the needs of clients and families, which can each be considered a unique set of capabilities and requirements—a set of information inputs to the process. These needs may be articulated formally, for example, via a set of scores from standardized measurements, or informally, as subjective observations of caregivers. In any case, the needs embody knowledge about functional and social goals, physical and cognitive capacities, preferences, occupational activities, cultural environments, and other personal/ environmental factors of relevance to the child and family. This knowledge about the client's needs permeates through the ecosystem, initially driving systematic knowledge generation via the scientific method (discovery phase), followed by knowledge generation via development activities (invention phase), and finally knowledge creation via production methods (innovation phase).
The need-driven knowledge ecosystem invokes one or more communities of practice, which are fluid and evolving assemblies of individuals united by a common concern or passion. Figure 1 depicts the community of practice for the Infinity Communication Access Lab. This community is the superset of individuals involved in realizing the goals of discovery and translation. The team at the lab consists of an occupational therapist, a speech language pathologist, and a clinical engineer, all of whom work full-time in the lab.
Figure 1: Community of practice within which the Infinity Communication Access Lab is embedded
Figure 1 Extended Text Description [Select image to enlarge]
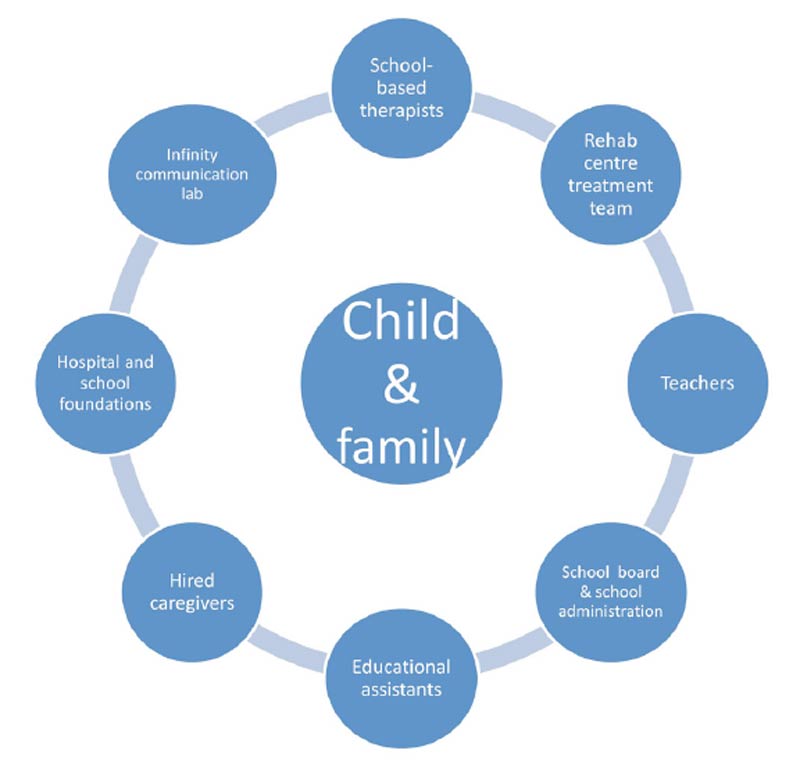
Source: © Infinity Communication Access Lab. SEDL used with permission.
The invoked community includes foundations that raise funds for lab activities, teachers and educational assistants who work daily with a child in the classroom setting, school-based therapists and the hospital-based treatment team who are involved in developing the child's communication skills and strategies, and of course, parents and caregivers who interact with the child in the home and community. By engaging all those who partake in the care and pedagogy of the child, the community-of-practice approach ensures that knowledge about the child's technology and communication strategies flows naturally among all the partners. In turn, these knowledge connections increase the consistency of communication with the child across settings and mitigate the risk of technology abandonment. The roles of the various parties are further elucidated in the next section.
The Collaborative Access Delivery and Training Protocol
Figure 2 summarizes the annual protocol of the lab. Each year, the lab engages a new cohort of 10 students at Sunny View Public School. The protocol entails three parallel streams of training: for students, for teachers, and for parents.
Figure 2: Access technology delivery protocol
Figure 2 Extended Text Description [Select image to enlarge]
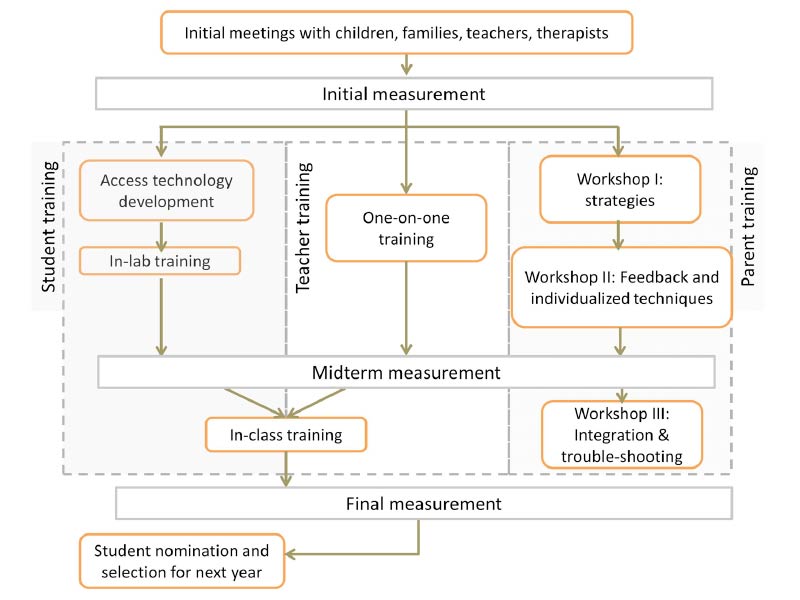
Source: © Infinity Communication Access Lab. SEDL used with permission.
Initial Assessment
Meetings are held with the student's family, educational staff, school therapists, and therapists from external agencies (where applicable) to gather information on the student's history with assistive technology use and to establish functional goals. These goals are incorporated into the student's Individualized Education Plan.
A client information questionnaire (Memarian, Venetsanopoulos, & Chau, 2011a) is administered to describe physical function, cognition, sensory acuity, motor skills, and communication skills. Collectively, this information guides the identification of potential access modalities (body parts, movements, or body processes) that require minimal user effort.
Development or Selection of Access Technology
Based on the initial assessment, primary and secondary (where appropriate) access modalities are identified. Corresponding access technologies are selected for or adapted to the child. Where no suitable technology exists, a custom access pathway is created using the library of sensing and processing tools available through the Bloorview Research Institute of the Holland Bloorview Kids Rehabilitation Hospital.
INITIAL MEASUREMENT. Prior to training, the staff captures a snapshot of the student's baseline communication, including the efficacy of the switch and a school function assessment, as well as the teacher's satisfaction with existing access technology (where applicable).
Student Training (Phase I). A customized switch training regimen is mapped out for each student (sixteen 30-minute one-on-one sessions with the Infinity Lab's occupational therapist). Sessions focus on initiating independent and appropriate switch activations, in addition to motor movement development (where applicable), timing, tracking, and scanning skills. To motivate students, games and activities are tailored to each child's individual preferences.
Educational Staff Training (Phase I). Teachers and educational assistants receive mentorship on developing communication partner skills and creating opportunities for incorporating access technologies and augmentative communication devices in the classroom. Initially, an interaction between the student and education staff is video-recorded. This video is reviewed with a speech language pathologist who provides and models individualized strategies to promote further communication development and technology integration in the classroom. These training sessions occur on a one-on-one basis with the Infinity Lab's speech language pathologist.
Parent Training. Parent training workshops are conducted at three separate times in the school year. Emphasis is placed on communication partner skill development: creating opportunities at home and in the community to integrate technology-mediated communication. The first workshop focuses on communication goals and strategies to increase communication at home. The second workshop collects feedback from parents regarding their child's progress as a result of the suggestions made in the first workshop and equips parents with additional individualized techniques. The final workshop discusses the integration of the communication technology at home and in the community and provides troubleshooting advice.
MIDTERM MEASUREMENT. After the first phase of student and teacher training (up to 8 weeks), the staff administers a battery of outcome measures to gauge progress toward achievement of identified goals (Goal Attainment Scaling), acquisition of communication skills, changes in school function, and improvements in switch efficacy.
Student and Educational Staff Training (Phase II). Once the student demonstrates efficient, independent, and meaningful use of his/her communication technology and the educational staff is armed with communication and classroom integration strategies, training migrates into the classroom. Up to sixteen 30-minute sessions take place in the classroom. During these sessions, the educational staff practices implementing communication enhancing strategies in multiple classroom situations with a speech language pathologist providing prompts and feedback as necessary.
FINAL MEASUREMENT. At the conclusion of Phase II training, the team re-administers the arsenal of measures to quantify goal attainment, gains in communication, changes in school function, and proficiency with technology use as well as the teacher's satisfaction with the technology.
Throughout the project, the lab team works closely with the school-based therapist and therapists from children treatment centers (where applicable) so that all parties are supporting the same functional communication goals throughout the year. Engagement of these clinicians from the initial assessment (described above), as well as their ad-hoc participation in student training and monthly or bimonthly meetings with the team, is an effective knowledge exchange arrangement. By the end of the school year, clinicians have adequate knowledge of the described activities to continue supporting the child's communication development via the new technology.
Creating Evidence Around Access Technologies
Figure 3 portrays some of the access technologies that have been developed and transferred into the schools and homes of various clients. These access technologies have been paired with voice output devices, on-screen keyboards, or tablet communication apps to create full communication solutions.
Figure 3: Examples of access technologies developed and deployed by the Infinity Communication Access Lab
a. Footnote 1
Figure 3a Extended Text Description [Select image to enlarge]

b. Footnote 2
Figure 3b Extended Text Description [Select image to enlarge]

c.
Figure 3c Extended Text Description [Select image to enlarge]

d.
Figure 3d Extended Text Description [Select image to enlarge]

Figure 3. Examples of access technologies developed and deployed by the Infinity Communication Access Lab: (a) vocal fold vibration device, (b) infrared facial thermographic switch, (c) multi-camera tongue switch, (d) mechanomyographic switch.
Source: © Infinity Communication Access Lab. SEDL used with permission.
Footnotes
- Footnote 1
-
Figure 3a: From "Neckband Turns Sound into Computer Clicks," by L. Kinross, April 5, 2010, BLOOM Magazine. Copyright 2010 by Holland Bloorview Kids Rehabilitation Hospital. Retrieved from http://bloom-parentingkidswithdisabilities.blogspot.com/2010/04/neckband-turns-corvins-sounds-into.html. SEDL reprinted with permission from Holland Bloorview Rehabilitation Hospital.
- Footnote 2
-
Figure 3b: From "Infrared Thermography as an Access Pathway for Individuals with Severe Motor Impairments," by N. Memarian, A. N. Venetsanopoulos, & T. Chau, 2009, Journal of NeuroEngineering and Rehabilitation, 6(11), p. 5. Copyright 2009 by Memarian et al. Retrieved from http://www.jneuroengrehab.com/content/6/1/11. SEDL used in compliance with Creative Commons Attribution License available at http://creativecommons.org/licenses/by/3.0 which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
For children who do not have functional speech but do have extant control of their vocal folds, staff developed the "hummer" (Figure 3a), a system that detects the vibrations of the vocal folds associated with silent humming (Falk, Chan, Duez, Teachman, & Chau, 2010; Lui, Falk, & Chau, 2012). For an individual who only retained voluntary opening and closing of his mouth, the Infinity Lab developed an infrared thermographic system that detects this motion non-invasively (Memarian, Venetsanopoulos, & Chau, 2011a, 2011b). This solution (Figure 3b) was implemented in the client’s home through the support of IBM. Some children exemplify well- controlled tongue movements amid widespread muscle spasticity or hyperkinetic movements. Figure 3c depicts a school and home-based solution that uses multiple web cameras to capture voluntary tongue protrusions (Leung & Chau, 2010), admitting varying head postures. Finally, in Figure 3d, a child models a mechanomyographic access system (Alves & Chau, 2010, 2011) that mechanically detects voluntary muscle contractions. This technology facilitates the functional use of small, deep, or atrophied muscles.
In all cases, the philosophy of enabling eventual assistive technology implementation has served to create a solid base of scientific evidence around access technologies that have been successful for each individual client. Within the parameters of available resources, the team leaves no case unpublished. While knowledge generated from rigorous experimentation and performance measurement is necessary for scientific papers, the staff also makes significant efforts to capture the associated practice wisdom, valuable knowledge that derives primarily from practical experience and usually remains tacit and undocumented. This type of “networked knowledge,” that is, knowledge that arises from interactions among individuals, flourishes in a community of practice. From experience in the Infinity Lab, it is the combined translation of traditional research knowledge and community-generated wisdom that ultimately facilitates the functional use of access technologies in real environments.
Program Summary
The Infinity Communication Access Lab leverages available resources to provide full support to both children and their families. By utilizing a three-step need-driven assessment program, the Infinity Lab is able to deliver continued training and guidance to students, parents, and educational staff. This experience in creating effective and evidence-based access technologies allows the lab not only to contribute to the scientific research knowledge base but also to further the abilities of the students who need these access technologies. By individualizing the process and creating access technology where needed, the Infinity Communication Access Lab shows its dedication to the success of each student.
The Infinity Communication Access Lab received a monetary award in the amount of $1,000 for providing detailed information to the KT4TT on their exemplary practices and for allowing the KT4TT to showcase their 'best practice' product development approaches to the broader NIDILRR community. In FOCUS Technical Brief No. 30, the KT4TT showcased the consumer involvement best practices of CreateAbility Concepts, Inc. (CCI), a SBIR Phase II NIDILRR grantee, as well as how the RERC-ACT leveraged available resources from their host institution, the University of Colorado, in utilizing the business and technology transfer expertise of their University's Technology Transfer Office (Leahy, 2011). The KT4TT continues to identify and highlight projects sponsored by NIDILRR/USDE or other agencies, demonstrating exemplary practices in the development, transfer, and production of assistive technology, thus ensuring that their research and development outputs deliver beneficial outcomes for people with disabilities.
References
Alves, N., & Chau, T. (2010). The design and testing of a novel mechanomyogram-driven switch controlled by small eyebrow movements. Journal of NeuroEngineering and Rehabilitation. 7, 22. doi:10.1186/1743-0003-7-22 http://www.jneuroengrehab.com/content/7/1/22
Alves, N., & Chau, T. (2011). Mechanomyography as an access pathway: corporeal contraindications. Disability and Rehabilitation: Assistive Technology, 6(6), 552-563.
Chau, T., Moghimi, S., & Popovic, M.R. (in press). Knowledge translation in rehabilitation engineering research and development: A knowledge ecosystem framework. Archives of Physical Medicine and Rehabilitation.
Falk, T. H., Chan, J., Duez, P., Teachman, G., & Chau, T. (2010). Augmentative communication based on realtime vocal cord vibration detection. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 18(2), 159-163.
Lane, J. P., & Flagg, J. L. (2010). Translating three states of knowledge–Discovery, invention and innovation. Implementation Science, 5(1). doi:10.1186/1748- 5908-5-9 http://www.implementationscience.com/content/5/1/9
Leahy, J. A. (2011). KT4TT: Knowledge translation embedded in technology transfer. FOCUS Technical Brief (30). Austin, TX: SEDL, National Center for the Dissemination of Disability Research.
Leung, B., & Chau, T. (2010). A multiple camera tongue switch for a child with severe spastic quadriplegic cerebral palsy. Disability and Rehabilitation: Assistive Technology, 5(1), 58-68.
Lui, M., Falk, T., & Chau, T. (2012). Development and evaluation of a dual-output vocal cord vibration switch for persons with multiple disabilities. Disability and Rehabilitation: Assistive Technology, 7(1), 82-88.
Memarian, N., Venetsanopoulos, A. N., & Chau, T. (2011a). Body functions and structures pertinent to infrared thermography-based access for clients with severe motor disabilities. Assistive Technology, 23(2), 53-64.
Memarian, N., Venetsanopoulos, A. N., & Chau, T. (2011b). Client-centred development of an infrared thermal access switch for a young adult with severe spastic quadriplegic cerebral palsy. Disability and Rehabilitation: Assistive Technology, 6(2), 179-187.
PRODUCT UTILIZATION SUPPORT AND HELP (PUSH) AWARD
The Center on Knowledge Translation for Technology Transfer (KT4TT) Product Utilization Support and Help (PUSH) Award is a peer-to-peer dissemination activity based on the identification and distribution of 'best practice' approaches to development, transfer and/or production processes by researchers and technology grantees. The goal is to provide the broader research and NIDILRR community with exemplars of research utilization that have been proven effective.
The PUSH program is modeled after some elements of SEDL's highly successful Research Utilization Support & Help (RUSH) program. RUSH supported NIDILRR grantees in their efforts to get their NIDILRR-funded research findings used in targeted, measurable ways. PUSH candidates are university researchers or NIDILRR technology grantees identified by KT4TT staff as conducting meritorious activity in Technology Transfer (TT) or Knowledge Translation (KT) for TT. The KT4TT, in conjunction with the selected candidate, generates a brief evidence-based description of a carrier used to successfully overcome a barrier within the technology transfer process. The supporting evidence may include research and/or practice knowledge.
CENTER ON KT4TT
The 5-year Center on Knowledge Translation for Technology Transfer (KT4TT) project (http://publichealth.buffalo.edu/cat/kt4tt.html) was awarded to the University at Buffalo (SUNY), Center for Assistive Technology (CAT) on October 1, 2008. SEDL and Western New York Independent Living, Inc., are partners in the project. SEDL's role focuses on utilization-oriented methods of dissemination, training, and technical assistance to effectively communicate with knowledge producers and knowledge users. This FOCUS Technical Brief is a product of the SEDL-KT4TT partnership.
The project focuses on three key outcomes:
- Improved understanding of the barriers preventing successful knowledge translation for technology transfer and ways to overcome these barriers
- Advanced knowledge of best models, methods, and measures of knowledge translation and technology transfer for achieving outcomes
- Increased utilization of these validated best practices by NIDILRR's technology-oriented grantees
Center on Knowledge Translation for Technology Transfer
Acknowledgments
The authors gratefully acknowledge colleagues who contributed to the concepts expressed herein. This document is a product of the Center on Knowledge Translation for Technology Transfer (KT4TT) and is published by SEDL. KT4TT is funded under Grant H133A080050 by the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR) of the U.S. Department of Education. The opinions contained in this publication are those of the authors, and you should not assume endorsement by the federal government.
Recommended Citation
Leahy, J. A., & Chau, T. (2013). Infinity Communication Access Lab recognized with 2012 Product Utilization Support and Help (PUSH) Award. FOCUS Technical Brief (36). Austin, TX: SEDL, Disability Research to Practice Program.
Address Correspondence
James A. Leahy
Co-PI, Project Administrative Officer
Center on Knowledge Translation for Technology Transfer (KT4TT)
Center for Assistive Technology, University at Buffalo (SUNY)
100 Sylvan Parkway, Suite 400
Amherst, NY 14228
716-204-8606
Fax: 716-204-8610
E-mail: jimleahy@buffalo.edu
Authors
James A. Leahy, BS, is a co-principal investigator for the Center on Knowledge Translation for Technology Transfer at the University at Buffalo. Prior to his current position, Mr. Leahy was a co-principal investigator and director of commercialization for the Rehabilitation Engineering Research Center on Technology Transfer (T2RERC). He has demonstrated success in creating research and development partnerships between major corporations and other institutions in the academic sector.
Tom Chau, PhD, PEng, is vice president of research and director of the Bloorview Research Institute, Holland Bloorview Kids Rehabilitation Hospital, University of Toronto. Dr. Chau is also the Canada Research Chair in Pediatric Rehabilitation Engineering as well as a professor at the Institute of Biomaterials and Biomedical Engineering, University of Toronto.
Copyright © 2021 by SEDL
FOCUS: A Technical Brief is published by SEDL's Disability Research to Practice Program for the Center on Knowledge Translation for Technology Transfer (KT4TT). The contents of this document do not necessarily represent the policy of the U.S. Department of Education, and you should not assume endorsement by the federal government.
DISABILITY RESEARCH TO PRACTICE
Advancing Research, Improving Education
SEDL is an equal employment opportunity/affirmative action employer and is committed to affording equal access to education and employment opportunities for all individuals. SEDL does not discriminate on the basis of age, sex, race, color, creed, religion, national origin, sexual orientation, marital or veteran status, or the presence of a disability.
Available in alternate formats upon request. Available online: https://ktdrr.org/ktlibrary/articles_pubs/focus36
- Last Updated: